Hepatitis A (inactivated) and hepatitis B (rDNA) vaccine (adsorbed).
1 dose (1 ml) contains: Hepatitis A virus (inactivated)1,2 720 ELISA Units; Hepatitis B surface antigen3,4 20 micrograms.
1 Produced on human diploid (MRC-5) cells.
2 Adsorbed on aluminium hydroxide, hydrated 0.05 milligrams Al3+.
3 Produced in yeast cells (Saccharomyces cerevisiae) by recombinant DNA technology.
4 Adsorbed on aluminium phosphate 0.4 milligrams Al3+.
The vaccine may contain traces of neomycin which is used during the manufacturing process (see Contraindications).
Excipients/Inactive Ingredients: Sodium chloride, Water for injections.
Pharmacotherapeutic group: Hepatitis vaccines. ATC code: J07BC20.
Pharmacology: Pharmacodynamics: Twinrix Adult is a combined vaccine formulated by pooling bulk preparations of the purified, inactivated hepatitis A (HA) virus and purified hepatitis B surface antigen (HBsAg), separately adsorbed onto aluminium hydroxide and aluminium phosphate. The HA virus is propagated in MRC5 human diploid cells. HBsAg is produced by culture, in a selective medium, of genetically engineered yeast cells.
Twinrix Adult confers immunity against HAV and HBV infection by inducing specific anti-HAV and anti-HBs antibodies.
Protection against hepatitis A and hepatitis B develops within 2-4 weeks. In the clinical studies, specific humoral antibodies against hepatitis A were observed in approximately 94% of the adults one month after the first dose and in 100% one month after the third dose (i.e. month 7). Specific humoral antibodies against hepatitis B were observed in 70% of the adults after the first dose and approximately 99% after the third dose.
The 0, 7 and 21 day primary schedule plus a fourth dose at month 12 is for use in exceptional circumstances in adults. In a clinical trial where Twinrix Adult was administered according to this schedule, 82% and 85% of vaccinees had seroprotective levels of anti-HBV antibodies at 1 and 5 weeks respectively following the third dose (i.e. at months 1 and 2 after the initial dose).
The seroprotection rate against hepatitis B increased to 95.1% by three months after the first dose.
Seropositivity rates for anti-HAV antibodies were 100%, 99.5% and 100% at months 1, 2 and 3 after the initial dose. One month after the fourth dose, all vaccinees demonstrated seroprotective levels of anti-HBs antibodies and were seropositive for anti-HAV antibodies.
In a clinical study conducted in subjects over 40 years of age, the seropositivity rate for anti-HAV antibodies and seroprotection rate against hepatitis B of Twinrix Adult following a 0, 1, 6 months schedule were compared with the seropositivity and seroprotection rates of monovalent hepatitis A and B vaccines when administered in opposite arms.
The seroprotection rate against hepatitis B after the administration of Twinrix Adult was 92% and 56% at 7 and 48 months respectively, versus 80% and 43% after the GlaxoSmithKline Biologicals monovalent 20 μg hepatitis B vaccine, and 71% and 31% after another licensed monovalent 10 μg hepatitis B vaccine. Anti-HBs antibody concentrations decreased as age and body mass index increased; they were also lower in male than in female subjects.
The seropositivity rate for anti-HAV antibodies after Twinrix Adult was 97% at both 7 and 48 months versus 99% and 93% after the GlaxoSmithKline Biologicals monovalent hepatitis A vaccine and 99% and 97% after another licensed monovalent hepatitis A vaccine.
Subjects received an additional dose of the same vaccine(s) 48 months after the first dose of the primary vaccination course. One month after this dose, 95% of the subjects vaccinated with Twinrix Adult achieved seroprotective levels of anti-HBV antibodies (≥10 mIU/ml).
In two long-term clinical studies conducted in adults aged 17 years to 43 years, respectively 18 and 25 subjects had evaluable tests 20 years after the primary vaccination with Twinrix Adult; the anti-HAV seropositivity rates were 100% and 96% respectively and the anti-HBs seroprotection rates were 94% and 92%, respectively.
Pharmacokinetics: Evaluation of pharmacokinetic properties is not required for vaccines.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on general safety studies.
Twinrix Adult is indicated for use in non-immune adults and adolescents 16 years of age and above who are at risk of both hepatitis A and hepatitis B infection.
Posology: Dosage: A dose of 1.0 ml is recommended for adults and adolescents 16 years of age and above.
Primary vaccination schedule: The standard primary course of vaccination with Twinrix Adult consists of three doses, the first administered at the elected date, the second one month later and the third six months after the first dose.
In exceptional circumstances in adults, when travel is anticipated within one month or more after initiating the vaccination course, but where insufficient time is available to allow the standard 0, 1, 6 month schedule to be completed, a schedule of three intramuscular injections given at 0, 7 and 21 days may be used. When this schedule is applied, a fourth dose is recommended 12 months after the first dose.
The recommended schedule should be adhered to. Once initiated, the primary course of vaccination should be completed with the same vaccine.
Booster dose: Long-term antibody persistence data following vaccination with Twinrix Adult are available up to 20 years after vaccination (see Pharmacology: Pharmacodynamics under Actions). The anti-HBs and anti-HAV antibody titres observed following a primary vaccination course with the combined vaccine are in the range of what is seen following vaccination with the monovalent vaccines. General guidelines for booster vaccination can therefore be drawn from experience with the monovalent vaccines.
Hepatitis B: The need for a booster dose of hepatitis B vaccine in healthy individuals who have received a full primary vaccination course has not been established; however some official vaccination programmes currently include a recommendation for a booster dose of hepatitis B vaccine and these should be respected.
For some categories of subjects or patients exposed to HBV (e.g., haemodialysis or immunocompromised patients) a precautionary attitude should be considered to ensure a protective antibody level ≥10 IU/l.
Hepatitis A: It is not yet fully established whether immunocompetent individuals who have responded to hepatitis A vaccination will require booster doses as protection in the absence of detectable antibodies may be ensured by immunological memory. Guidelines for boosting are based on the assumption that antibodies are required for protection.
In situations where a booster dose of both hepatitis A and hepatitis B are desired, Twinrix Adult can be given. Alternatively, subjects primed with Twinrix Adult may be administered a booster dose of either of the monovalent vaccines.
Method of administration: Twinrix Adult is for intramuscular injection, preferably in the deltoid region.
Exceptionally the vaccine may be administered subcutaneously in patients with thrombocytopenia or bleeding disorders. However, this route of administration may result in suboptimal immune response to the vaccine (see Precautions).
Cases of overdose have been reported during post-marketing surveillance. Adverse events reported following overdosage were similar to those reported with normal vaccine administration.
Hypersensitivity to the active substances or to any of the excipients listed in Description or neomycin.
Hypersensitivity after previous administration of hepatitis A and/or hepatitis B vaccines.
The administration of Twinrix Adult should be postponed in subjects suffering from acute severe febrile illness.
Syncope (fainting) can occur following, or even before, any vaccination especially in adolescents as a psychogenic response to the needle injection. This can be accompanied by several neurological signs such as transient visual disturbance, paraesthesia and tonic-clonic limb movements during recovery. It is important that procedures are in place to avoid injury from faints.
It is possible that subjects may be in the incubation period of a hepatitis A or hepatitis B infection at the time of vaccination. It is not known whether Twinrix Adult will prevent hepatitis A and hepatitis B in such cases.
The vaccine will not prevent infection caused by other agents such as hepatitis C and hepatitis E and other pathogens known to infect the liver.
Twinrix Adult is not recommended for postexposure prophylaxis (e.g. needle stick injury).
The vaccine has not been tested in patients with impaired immunity. In haemodialysis patients and persons with an impaired immune system, adequate anti-HAV and anti-HBs antibody titres may not be obtained after the primary immunisation course and such patients may therefore require administration of additional doses of vaccine.
Obesity (defined as BMI ≥30 kg/m2) has been observed to reduce the immune response to hepatitis A vaccines. A number of factors have been observed to reduce the immune response to hepatitis B vaccines. These factors include older age, male gender, obesity, smoking, route of administration, and some chronic underlying diseases. Consideration should be given to serological testing of those subjects who may be at risk of not achieving seroprotection following a complete course of Twinrix Adult. Additional doses may need to be considered for persons who do not respond or have a sub-optimal response to a course of vaccinations.
As with all injectable vaccines, appropriate medical treatment and supervision should always be readily available in case of a rare anaphylactic event following the administration of the vaccine.
Since intradermal injection or intramuscular administration into the gluteal muscle could lead to a suboptimal response to the vaccine, these routes should be avoided. However, exceptionally Twinrix Adult can be administered subcutaneously to subjects with thrombocytopenia or bleeding disorders since bleeding may occur following an intramuscular administration to these subjects (see Dosage & Administration).
Twinrix Adult should under no circumstances be administered intravascularly.
As with any vaccine, a protective immune response may not be elicited in all vaccinees.
Traceability: In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded.
Effects on ability to drive and use machines: Twinrix Adult has no or negligible influence on the ability to drive and use machines.
Pregnancy: The effect of Twinrix Adult on embryo-fetal, peri-natal and post-natal survival and development has been assessed in rats. This study did not indicate direct or indirect harmful effects with respect to fertility, pregnancy, embryonal/fetal development, parturition or post-natal development.
The effect of Twinrix Adult on embryo-fetal, peri-natal and post-natal survival and development has not been prospectively evaluated in clinical trials.
Data on outcomes of a limited number of pregnancies in vaccinated women do not indicate any adverse effects of Twinrix Adult on pregnancy or on the health of the fetus/newborn child. While it is not expected that recombinant hepatitis B virus surface antigen would have adverse effects on pregnancies or the fetus it is recommended that vaccination should be delayed until after delivery unless there is an urgent need to protect the mother against hepatitis B infection.
Breast-feeding: It is unknown whether Twinrix Adult is excreted in human breast milk. The excretion of Twinrix Adult in milk has not been studied in animals. A decision on whether to continue/discontinue breast-feeding or to continue/discontinue therapy with Twinrix Adult should be made taking into account the benefit of breast-feeding to the child and the benefit of Twinrix Adult therapy to the woman.
Summary of the safety profile: The safety profile presented as follows is based on a pooled analysis of events per dose from more than 6,000 subjects who received either the standard 0, 1, 6 month schedule (n=5,683) or the accelerated 0, 7, 21 days schedule (n=320). The most commonly reported adverse reactions following Twinrix Adult administration with the standard 0, 1, 6 month schedule are pain and redness occurring in a per dose frequency of 37.6% and 17.0% respectively.
In the two clinical trials in which Twinrix Adult was administered at 0, 7, 21 days, overall solicited general and local symptoms were reported with the same categories of frequency as defined as follows. After a fourth dose given at month 12, the incidence of systemic and local adverse reactions was comparable to that seen after vaccination at 0, 7, 21 days.
In comparative studies, it was noted that the frequency of solicited adverse events following the administration of Twinrix Adult is not different from the frequency of solicited adverse events following the administration of the monovalent vaccines.
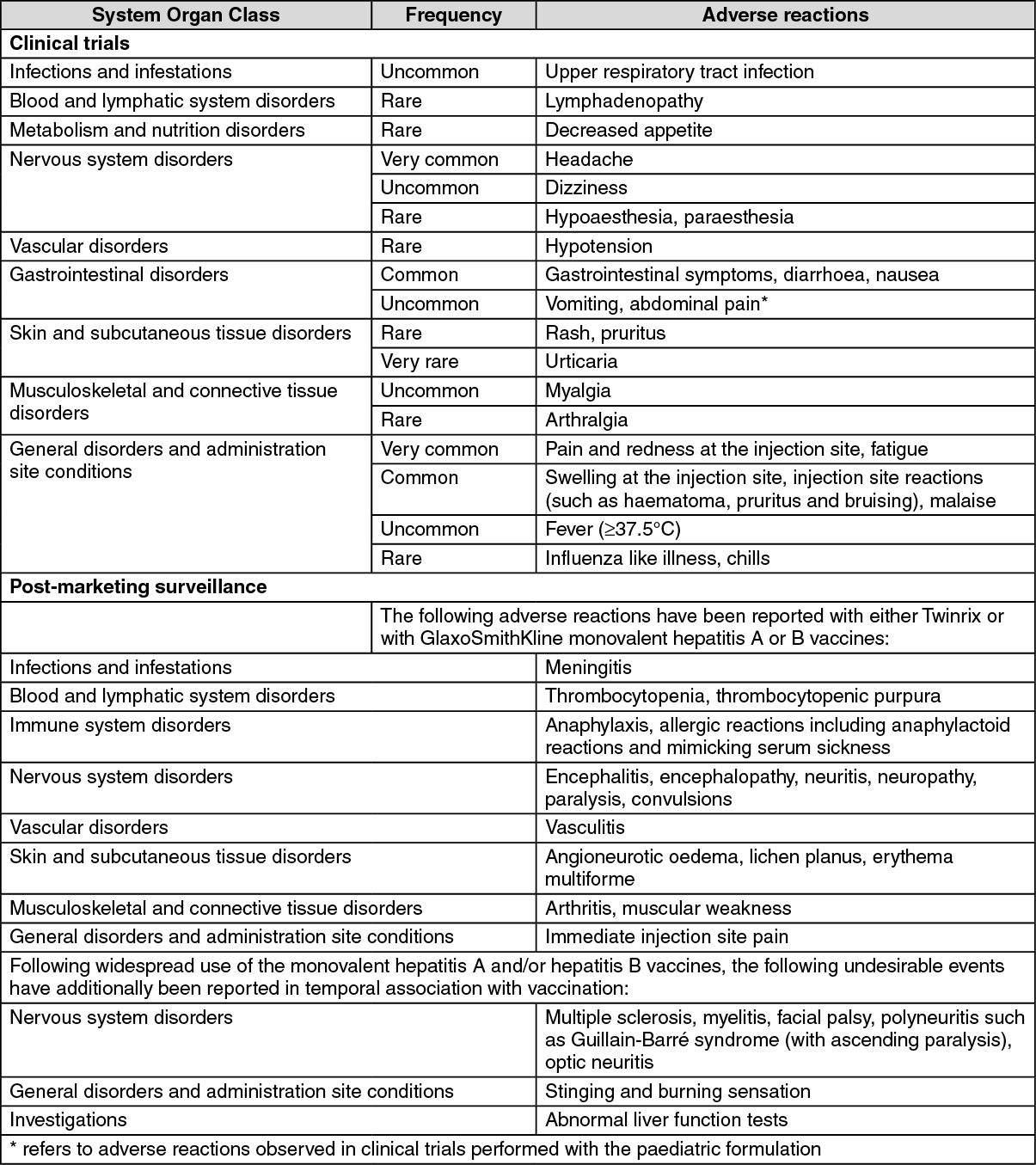
Tabulated list of adverse reactions: Frequencies are reported as: Very common ≥1/10; Common ≥1/100 to <1/10; Uncommon ≥1/1,000 to <1/100; Rare ≥1/10,000 to <1/1,000; Very rare <1/10,000. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
No data on concomitant administration of Twinrix Adult with specific hepatitis A immunoglobulin or hepatitis B immunoglobulin have been generated. However, when the monovalent hepatitis A and hepatitis B vaccines were administered concomitantly with specific immunoglobulins, no influence on seroconversion was observed although it may result in lower antibody titres.
Although the concomitant administration of Twinrix Adult and other vaccines has not specifically been studied, it is anticipated that, if different syringes and other injection sites are used, no interaction will be observed.
It may be expected that in patients receiving immunosuppressive treatment or patients with immunodeficiency, an adequate response may not be achieved.
Upon storage, a fine white deposit with a clear colourless layer above may be observed.
The vaccine should be re-suspended before use. When re-suspended, the vaccine will have a uniform hazy white appearance.
Re-suspension of the vaccine to obtain a uniform hazy white suspension: The vaccine should be re-suspended following the steps as follows.
1. Hold the syringe upright in a closed hand.
2. Shake the syringe by tipping it upside down and back again.
3. Repeat this action vigorously for at least 15 seconds.
4. Inspect the vaccine again: a. If the vaccine appears as a uniform hazy white suspension, it is ready to use - the appearance should not be clear.
b. If the vaccine still does not appear as a uniform hazy white suspension - tip upside down and back again for at least another 15 seconds - then inspect again.
The vaccine should be inspected visually for any foreign particulate matter and/or abnormal physical appearance prior to administration. In the event of either being observed, do not administer the vaccine.
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Incompatibilities: In the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products.
Store in a refrigerator (2°C - 8°C).
Do not freeze.
Store in the original package, in order to protect from light.
Shelf life: 3 years.
J07BC20 - combinations ; Belongs to the class of hepatitis viral vaccines.
Twinrix Adult vaccine (inj)
(pre-filled syringe) 1 mL x 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
